Cystic fibrosis–related liver disease

Cystic fibrosis (CF) can affect the health of your liver. Around 40% of adults with CF, and around 20% of children with CF show some liver changes. Around 20–25% of adults with CF, and just under 10% of children have liver disease.
-
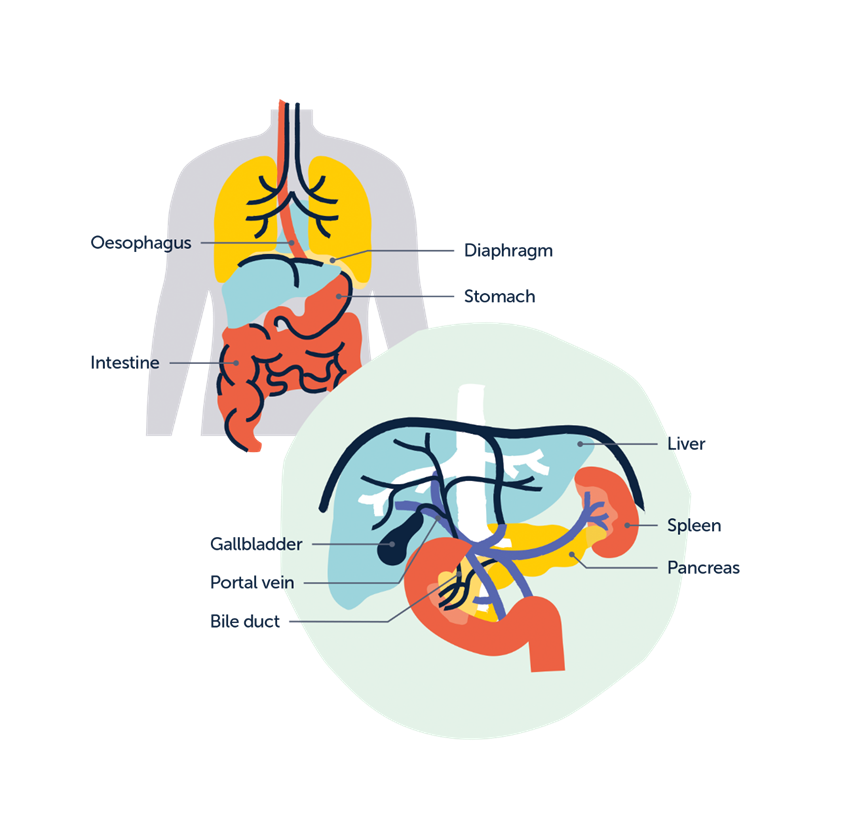
How a healthy liver looks and works
The liver is in the upper part of the abdomen, above the stomach. It sits just under the right-hand side of the diaphragm muscle, below the ribs.
The liver has many functions, including:
- processing digested food from the intestines
- producing bile, which helps your body digest fats
- controlling levels of fats, amino acids, and glucose in the blood
- breaking down food and turning it into energy
- helping to fight infections
- neutralising and destroying all drugs and toxins
- storing iron, vitamins, and other essential chemicals
- making, breaking down, and regulating many hormones, including sex hormones
- making proteins and enzymes that are essential for blood clotting and repairing tissues.
-
How CF affects the liver
In recent years, more people are being diagnosed with cystic fibrosis–related liver disease (CFLD). This is most likely because people with CF are having screening for liver disease from a younger age. It could also be because people with CF are now living to an older age. People tend to put on weight as they get older, and this can increase the chances of having CFLD.
People with CF can have liver disease because of:
- problems with bile draining from the liver via the bile ducts and gallbladder
- scarring in the liver, known as fibrosis and cirrhosis.
Bile ducts and gallbladder
The liver produces a liquid called bile. This helps your body to digest the fats you eat in food. Cystic fibrosis causes problems with how bile flows through the bile ducts. This is because the cells can’t transfer salts out of the cells effectively. In CF, bile becomes thicker and stickier. This can irritate and inflame the bile ducts. It can also block the bile ducts by forming gallstones. This can damage and scar the bile ducts.
Fibrosis and cirrhosis
Scarring, or fibrosis, can develop in the livers of people with CF. In severe cases, this can lead to cirrhosis. This is a more serious form of scarring. Cirrhosis is irreversible and can affect the way the liver works. Liver tissue becomes hard when it is scarred. This causes higher pressure in the portal vein – the major blood vessel flowing into the liver. This extra pressure can cause swollen blood vessels in the oesophagus and stomach. These are called varices. The spleen gets bigger because of the blood flowing back towards it. This is known as portal hypertension.
Fatty changes in the liver can also cause scarring. This is known as steatosis. Fat can irritate the liver and cause scarring. We don’t know why this happens. Other causes of fat in the liver include drinking too much alcohol.
-
Signs and symptoms of CF-related liver disease (CFLD)
Most people with CFLD have no signs or symptoms, or their symptoms are mild. You will have screening to check for CFLD. Children are screened from a young age.
If you have no symptoms, a diagnosis of CFLD can be based on:
- changes on a liver ultrasound scan
- mildly abnormal liver blood test results.
People with more advanced liver disease may have the following signs and symptoms.
Hepatomegaly
This means the liver is enlarged. Many people with CF have a mildly enlarged liver. This usually does not cause problems.
Splenomegaly
This means the spleen is enlarged. Splenomegaly develops when there is:
- scarring in the liver
- portal hypertension.
You may feel heaviness and swelling in the upper left side of the abdomen. In severe cases, this may extend across the abdomen.
Jaundice
Jaundice happens when bile can’t clear from the liver. The bile builds up in the blood and can show through the skin and urine instead.
People with jaundice have a yellowish colour to their skin and the whites of their eyes.
Jaundice can also cause:
- itching
- pale stools (poo)
- dark urine
- difficulty in digesting food
- a lack of energy
- trouble with concentrating.
In more advanced liver disease, jaundice is a sign of poor liver function.
Jaundice is also common if you get gallstones. This is because gallstones can block the bile from flowing out of the liver.
In rare cases, it can happen after developing a drug reaction, including to some antibiotics.
If you get jaundice, contact your CF team at once, and/or seek immediate medical attention.
Bleeding (bruising, nosebleeds and visible veins on the abdomen)
If the liver is scarred and you have portal hypertension, blood flow is redirected away from the liver. The blood flow goes to smaller blood vessels. These are more fragile and more likely to cause bleeding. It may also take longer for your blood to clot. This can raise the risk of bleeding.
People with portal hypertension and splenomegaly may also have a low platelet count. Platelets are blood cells that help the blood clot. So if you don’t have enough platelets, you have a higher risk of bleeding.
As well as more superficial bleeding with bruising and nosebleeds, people with portal hypertension can get varices. These mainly happen in the intestine (mostly in the oesophagus or stomach) and can bleed. If this happens, you may vomit blood or pass blood through the back passage. This can make stools (poo) look black and tarry.
If you notice blood in vomit or poo, contact your CF team or GP at once.
Problems with weight gain and muscle strength
The liver processes many nutrients from our food. Liver disease can stop the liver from absorbing fat and vitamins properly. This can make it harder to gain weight and build muscle. You may be more likely to get infections, including chest infections. You may also feel more tired.
Ascites
In advanced liver disease, excessive fluid may gather inside the abdomen. This is called ascites, and can cause bloating or a swollen abdomen. Ascites can also be a sign of portal hypertension.
-
How CFLD is diagnosed
You’ll have tests in a CF clinic to check:
- how your liver looks
- how your liver is working.
Ultrasound scan
An ultrasound (echo) liver scan checks the structure of the liver. The person doing the scan moves a probe gently across the skin over the liver. This is painless and only takes around ten minutes. Your doctor will look at the size of the liver and spleen together. This will tell them:
- if the bile ducts have become enlarged
- if there’s any evidence of gallstones.
They can also check the blood flow in the portal vein.
A new type of scan called a FibroScanÒ is now being used more often. It measures the amount of scarring and fat in the liver. This scan is also painless.
Magnetic resonance imaging (MRI) scan
An ultrasound scan may show stones in the bile ducts or gallbladder. If it does, you may need a more detailed MRI scan. This will look at the bile duct system. An MRI does not use any radiation. But you must lie very still during the tests. Young children sometimes need to be sedated for this.
Blood tests
You may need blood tests to check how your liver is working. These may include tests to measure bilirubin levels, liver enzymes, clotting, and vitamin levels.
Liver biopsy
In very rare cases, you may need a biopsy. You may have a biopsy:
- if your doctors aren’t sure if you have CFLD
- to make sure it’s not a different type of liver disease.
The person doing the biopsy uses an anaesthetic to numb the skin over the liver. They then briefly insert a needle into the liver to get a small sample. They use ultrasound to guide them while they do this. They then send the sample off for microscopic analysis.
If a child needs a biopsy, they will have sedation or a general anaesthetic (GA).
Nutrition and body-mass assessment
Malnutrition is a common problem in people with CFLD. It’s important to make sure you’re getting all the nutrients you need. Many people with advanced liver disease need nutritional support, such as tube feeding.
It’s important to look at nutrition as a whole. Your body weight might not tell doctors enough about your nutrition. So they may also measure your muscle mass. They may take skinfold measurement in your upper arms, or check your handgrip strength. These measurements tell them more about your muscle strength. DEXA scans look at bone density and can give information on your muscle mass.
Liver disease can also make fat malabsorption worse. It’s important to regularly review pancreatic enzyme (Creon) dosing. This is to make sure you are absorbing fat well.
Endoscopy
It is important to check for varices in the gut if:
- the blood pressure in the portal vein is raised
- the spleen is enlarged.
For some people, this may mean having an endoscopy once a year. This test uses an endoscope. This is a long, thin tube with a light and camera at one end. Your doctor uses it to look down the oesophagus (the gullet, or food pipe) and into the stomach to check for varices.
If your doctor finds any varices, they can treat them to stop blood from leaking out. They loop and tie tiny bands around the blood vessels during the endoscopy. This is called banding.
If a child needs an endoscopy, they will have it under GA.
Sometimes gallstones may get stuck in the bile duct. If this happens, you’ll need an endoscopy of the bile duct. This is called an endoscopic retrograde cholangiography (ERC). You usually have this in a specialist centre under GA.
If you have acute bleeding from varices, you will need to be admitted to hospital as an emergency. You will need an urgent endoscopy to look for the source of bleeding and treat it.
-
How CFLD is monitored
Most children with CF have blood tests at their annual review to check their liver works well. Sometimes they also have a baseline ultrasound scan.
In many adult CF centres, you may see both a CF specialist and a liver specialist (hepatologist) in one clinic.
If you start a new CFTR modulator, you will have blood tests every 3 months. You will then move on to blood tests once a year. But if they show problems with your liver, you may have them more often.
-
How CFLD is treated
Urso®
You may have a drug called ursodeoxycholic acid (also known as Urso® or UDCA). It has been used to treat people with significant CFLD for years. It occurs naturally in small amounts in bile. It can change the composition of bile. This helps bile flow through the liver more easily. Urso® can sometimes improve symptoms and liver blood tests. But we don’t yet know if it helps in the long term.
In the UK, Urso® tablets come in three strengths: 150mg, 250mg and 300mg. For smaller children, it is also available as a liquid. Children and adults can both have this drug. It is usually well tolerated. But in rare cases it may cause itching, rashes, nausea, vomiting or diarrhoea.
Vitamin K
CFLD can stop the liver from making enough clotting factors. This means:
- your blood won’t clot as easily
- you may have problems with bleeding.
In some cases, taking Vitamin K tablets daily may help.
Liver disease can also stop you absorbing enough of some vitamins in food. If this happens, you’ll need to take supplements. Most people with CF already take vitamin supplements. If you have CFLD, you’ll also take Vitamin K.
Endoscopy/surgery
You may have regular endoscopies with banding if you have:
- bleeding from the intestine
- portal hypertension
- advanced liver disease.
If you still have bleeding from varices after this treatment, your team may consider a transhepatic intrajugular portosystemic shunt (TIPS). You have this under general anaesthetic. Doctors place a tube called a stent into your liver. The stent connects the portal vein and the larger veins that drain blood to the heart. This reduces pressure in the portal vein. TIPS is suitable for older children and adults.
If you have portal hypertension, there are several drugs that might help. The most common one is carvedilol. It lowers blood pressure in and around the liver.
Liver transplants
If liver disease progresses, complications such as liver failure may develop. In these cases, doctors may consider a liver transplant. CF-related liver problems usually show up by late childhood. So some children who are still under a paediatric team may need liver transplants.
The outlook after a liver transplant is good. But it can be hard to decide the best timing for it. Your CF team and the liver unit team will work together to give you the best advice. A liver transplant will give you a new, working liver. But you’ll also need to take immunosuppressive medicine for the rest of your life. This is to stop your body from rejecting the organ.
-
What can I do to stay well?
You can’t stop CFLD from developing. But you can take steps to protect your liver and stay well. You should:
- avoid drinking too much alcohol. The NHS has guidelines to help you calculate alcohol units. You can also read our Drinking alcohol and cystic fibrosis leaflet.
- try to eat a balanced diet. The NHS has guidelines on how to eat a balanced diet. You can also take a look at our series of nutrition leaflets.
- try to get some exercise, if you are able to. The NHS has exercise guidelines and workouts to help improve your fitness and wellbeing. Your physiotherapy team can help you choose the best types of exercise for you.
-
Outlook for people with CFLD
Most people with CF who have liver problems generally have a very good outlook. For most people, liver problems won’t get worse over time. Or there will only be small changes. In these cases, you’ll just need a clinic review once a year. You’ll have a scan and blood tests at the review. Careful monitoring and treatment can manage complications. A small minority of people do get worse and need a transplant.
-
Additional reading
The Child Liver Disease Foundation has developed a leaflet for families affected by CFLD.
-
How we can support you
Our Helpline is open 10am to 4pm, Monday to Friday. It’s available to anyone looking for information or support with any part of cystic fibrosis, a listening ear, or just to talk things through.
How to reach us
- Call 0300 373 1000 or 020 3795 2184
- Email [email protected]
- Chat with us on Facebook, Twitter or Instagram
- Message us on WhatsApp on 07361 582053
-
Other formats
Download this information as a PDF
You can also ask for this resource in large print or as a text file by emailing [email protected].
We welcome your feedback on our resources. Please get in touch at [email protected].
This information was originally written by Dr David Honeybourne, Consultant Physician, Birmingham Heartlands Hospital and Dr Marianne Samyn, Consultant in Paediatric Hepatology, Kings College Hospital, London. February 2011. Reviewed by Dr Marianne Samyn in January 2017. Reviewed and updated by Dr Deepak Joshi, Consultant Hepatologist, and Dr Michael Waller, Consultant in Adult Cystic Fibrosis and Respiratory Medicine, King’s College Hospital NHS Foundation Trust, 2025.
A warm thank you to the CF clinical professionals and people with CF who helped us develop this information.
Last reviewed: July 2025
Next review due: January 2029
Our resources are free to download and order, but we would be very grateful if you would consider making a donation to help us continue our important work.
You might also be interested in
Information resources
We produce lots of information which covers a whole range of issues that can affect people living with cystic fibrosis (CF).
What is CF?
Cystic fibrosis, or CF, affects the lungs, digestive system and other organs. There are over 11,000 people living with it in the UK.
Here to help
If you’re worried about any aspect of CF, our Helpline is here to support you.